There are a few everyday life experiences that everybody is destined to go through every now and then. Like correctly plugging a USB device only at the third attempt (despite there are only two possibilities), or directly setting the alarm clock half an hour earlier because we know we’re used to putting it off at least four times, or having Mallet Finger.
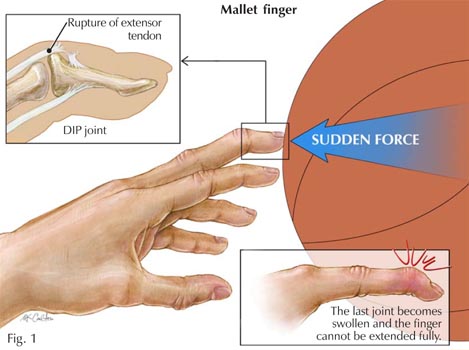
Mallet Finger is probably one of the most painful and annoying injuries of all time. Technically, it is an injury of the extensor digitorum tendon of the fingers at the distal interphalangeal joint (DIP). In more simple terms, it is the typical injury that occurs when we play basketball and the ball suddenly hits our extended finger. Besides the immediate sensation of pain, within a few minutes our finger will start swelling and we won’t be able to straighten it for a while. We then leave the court with an awesome facial expression (it really hurts, you all know…), but do we know what happened inside our finger?
 The distal interphalangeal joint (DIP)
The distal interphalangeal joint (DIP)  of the hand is nothing more than a hinge joint between the two last phalanges of the finger. This kind of joint only admits one degree of freedom, which is the rotation about the joint axis. As a result, our phalanges are allowed to make flexion and extension movements. Thus, the DIP is the last joint of the finger. A sudden high force acting at the tip of the finger (the ball we were trying to catch) strongly solicits the thin DIP extensor tendon. In case of rupture, or tearing, of this tendon from the bone, the finger usually gets painful, swollen, and bruised. Occasionally, blood can collect beneath the nail. In the worst case, the force of the blow may even pull away a piece of bone along with the tendon.
of the hand is nothing more than a hinge joint between the two last phalanges of the finger. This kind of joint only admits one degree of freedom, which is the rotation about the joint axis. As a result, our phalanges are allowed to make flexion and extension movements. Thus, the DIP is the last joint of the finger. A sudden high force acting at the tip of the finger (the ball we were trying to catch) strongly solicits the thin DIP extensor tendon. In case of rupture, or tearing, of this tendon from the bone, the finger usually gets painful, swollen, and bruised. Occasionally, blood can collect beneath the nail. In the worst case, the force of the blow may even pull away a piece of bone along with the tendon.  The loss of extensor tendon continuity might lead to severe consequences and must be carefully treated. In a first moment, ice should be immediately applied and the hand should be elevated above the level of the heart. Medical attention should be sought within a week after injury. Most mallet finger injuries can be treated without surgery.
The loss of extensor tendon continuity might lead to severe consequences and must be carefully treated. In a first moment, ice should be immediately applied and the hand should be elevated above the level of the heart. Medical attention should be sought within a week after injury. Most mallet finger injuries can be treated without surgery.  Normally, X-rays are necessary in order to look for potential bone fractures or joint misalignment. The presence of blood beneath the nail and nail detachment may be a sign of nail bed laceration or open (compound) fracture. A splint can be applied to hold the fingertip straight (in extension) until it heals (8 weeks full-time, 3-4 further weeks less frequently). With this treatment plan, the finger usually regains an acceptable function and appearance. Despite that, it is not guaranteed that the patient will be able to regain full fingertip extension.
Normally, X-rays are necessary in order to look for potential bone fractures or joint misalignment. The presence of blood beneath the nail and nail detachment may be a sign of nail bed laceration or open (compound) fracture. A splint can be applied to hold the fingertip straight (in extension) until it heals (8 weeks full-time, 3-4 further weeks less frequently). With this treatment plan, the finger usually regains an acceptable function and appearance. Despite that, it is not guaranteed that the patient will be able to regain full fingertip extension.
If nonsurgical treatment fails, after  consultation with an orthopaedic surgeon the patient may consider to resort to surgical repair. In case of very severe deformity or inability to properly use the injured finger, surgery is done to repair the fracture using pins, pins and wire, or even small screws. Surgical treatment of the damaged tendon can include tightening the stretched tendon tissue, using tendon grafts, or even fusing the joint straight.
consultation with an orthopaedic surgeon the patient may consider to resort to surgical repair. In case of very severe deformity or inability to properly use the injured finger, surgery is done to repair the fracture using pins, pins and wire, or even small screws. Surgical treatment of the damaged tendon can include tightening the stretched tendon tissue, using tendon grafts, or even fusing the joint straight.
_
sources: mainly this website and this website, and then Google Images


 A friend of mine told me to have a look at this one: Virtual Knee Surgery. It is a very realistic game that follows all the basic steps of a Total Knee Replacement surgery. The user is invited to interact with the surgeon in order to perform the necessary operations.
A friend of mine told me to have a look at this one: Virtual Knee Surgery. It is a very realistic game that follows all the basic steps of a Total Knee Replacement surgery. The user is invited to interact with the surgeon in order to perform the necessary operations.
















